
“These are the sickest, the ones where over 40% will die……It’s the Uber driver, bus drivers, restaurant workers, delivery people, security guards. People think its old people dying. Everyone I’m looking after (in ICU) is in their 50’s and 60’s.”
These are the words of Dr Helen Simpson, Consultant Endocrinologist, who is volunteering in UCH Hospital Intensive Care Unit, quoted in the Guardian on 12 February 2021. Her words reflect what we have now long known about the pandemic: front-line essential workers, those who have kept the country going throughout, are much more exposed to Covid-19 and are dying at disproportionate rates than other workers.
The ONS recently released its updated report on Covid-19 related deaths by occupation (up to 28 December 2020). It paints a stark picture of high death rates for essential workers, who have had to go to work, many times higher than others who are able to work from home, such as senior managers, directors and professionals.
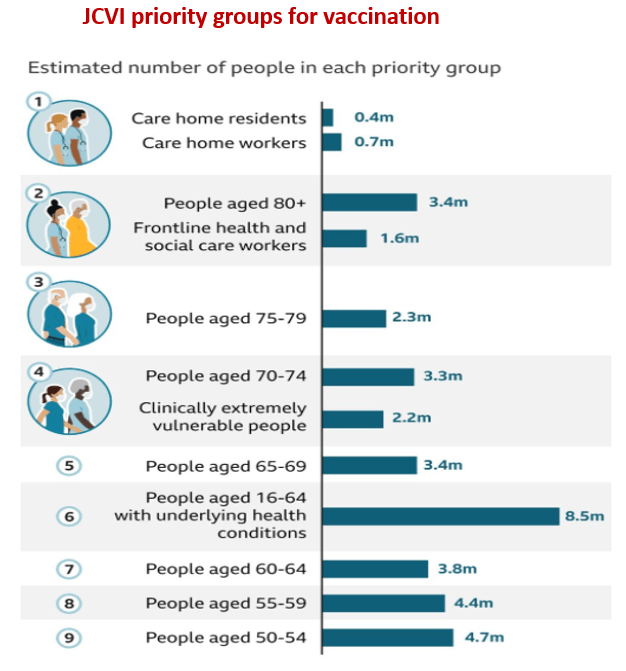
The ONS report is timely: it was published 2 days before the Joint Committee for Vaccination and Immunisation (JCVI) published its strategy for vaccinating the country against Covid-19, which has been endorsed by the government. Because of the initial shortage of vaccines, and the logistical challenges of vaccinating the entire adult population, the strategy is quite rightly based on prioritising those at greatest risk of dying. Age by far the greatest risk factor: people over 70 are at very high risk while those over 80 are at extremely high risk. Care home residents are a very high priority, as they are at very high risk. Health and social care workers have also been allocated high priority – they are at high risk of exposure to infection and of spreading the infection to those they care for. Next in line are those who are “clinically extremely vulnerable” (CEV), people with serious medical conditions such as cancer, immune disorders, organ transplants and severe disease of vital organs. The rationale for this is that CEV people have about the same risk of dying from Covid-19 as do people aged 70-79, from data from the first wave last year, according to the JCVI.
At the time of writing the vaccination programme has been very successful to date; it has vaccinated the great majority of people in the above categories, so called groups 1-4 of the JCVI priority list. However, it is very concerning that the rate of vaccination of BAME people within groups 1-4, is much less than the rate for whites, i.e. about half in some ethnic groups. BAME people are at considerably higher risk of dying of Covid-19 so this is especially worrying.
We are at the point now of beginning to vaccinate the next two priority groups in the JCVI’s list: group 5, who are people over 65 years of age, based on their “absolute increased risk” which is considered to be higher than the risk for those who have underlying health conditions, who constitute group 6. Groups 7, 8 and 9 are people aged 60-64, 55-59 and 50-55 years respectively. The rest of the population will be vaccinated after this.
The table below shows the priority groups, and the number of people in each group:
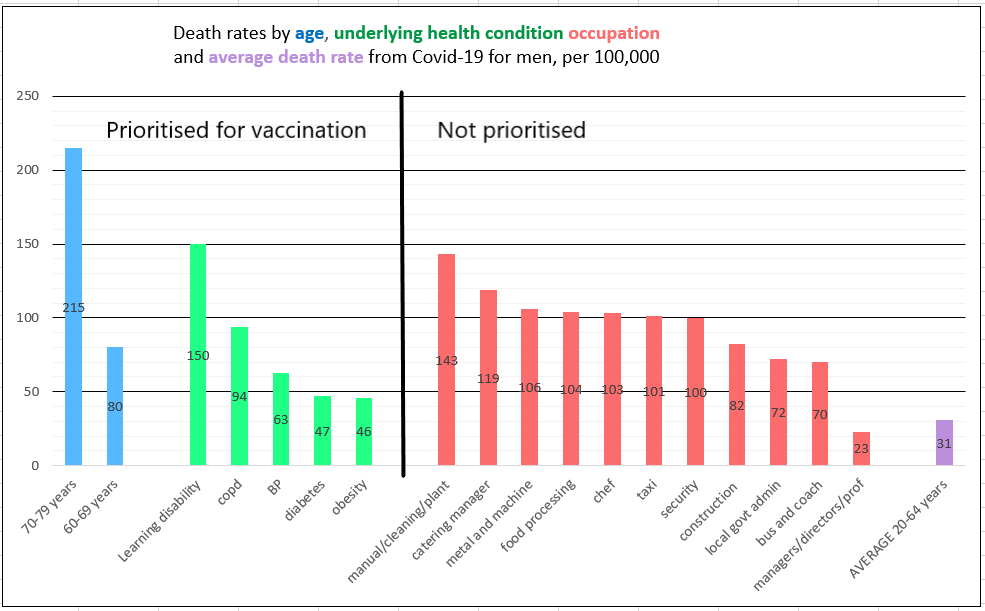
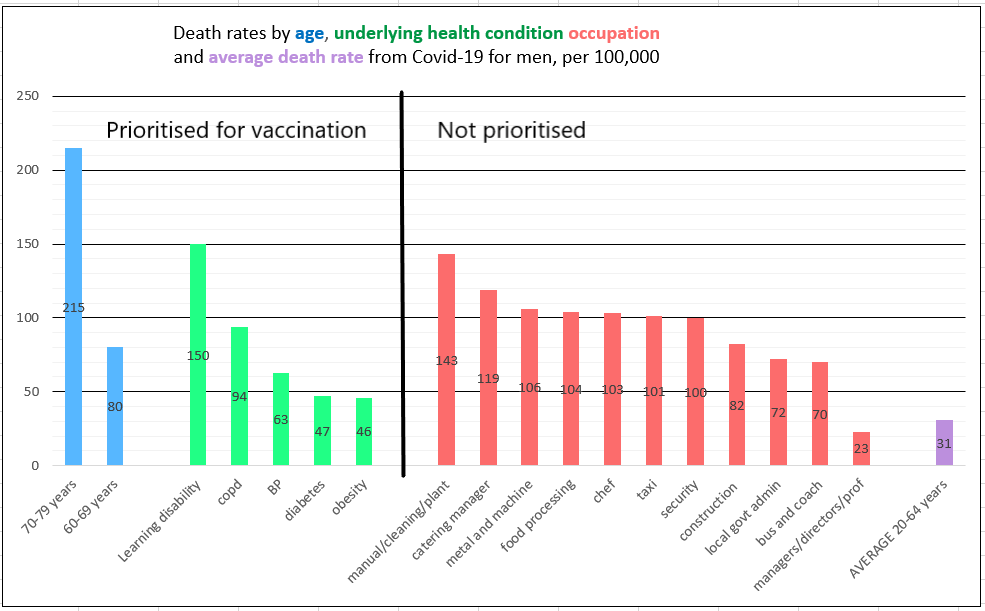
The problem is that when it comes to essential workers, the JCVI abandons the methodology of determining priority according to absolute increased risk of death. According to the death rates in the ONS report, many groups of essential workers have much higher absolute death rates than both people aged 65-69, and those aged 16-64 with underlying health conditions. This is especially true of male workers, while women working in essential jobs have risks roughly equal to those in priority groups 5 and 6. Some women workers however, ie, machinists in garment factories, have four times the average death rate. The graphs below illustrate the various deaths rates.
Please note health and social care workers, who are at high risk, are not included as they are already in the first four priority groups of people being vaccinated.
Death rates for essential workers (men) *
(average rate is in purple on right)
Death rates for essential workers (women) *
(please note the different Y-axis values, i.e. half of that in the graph for men)
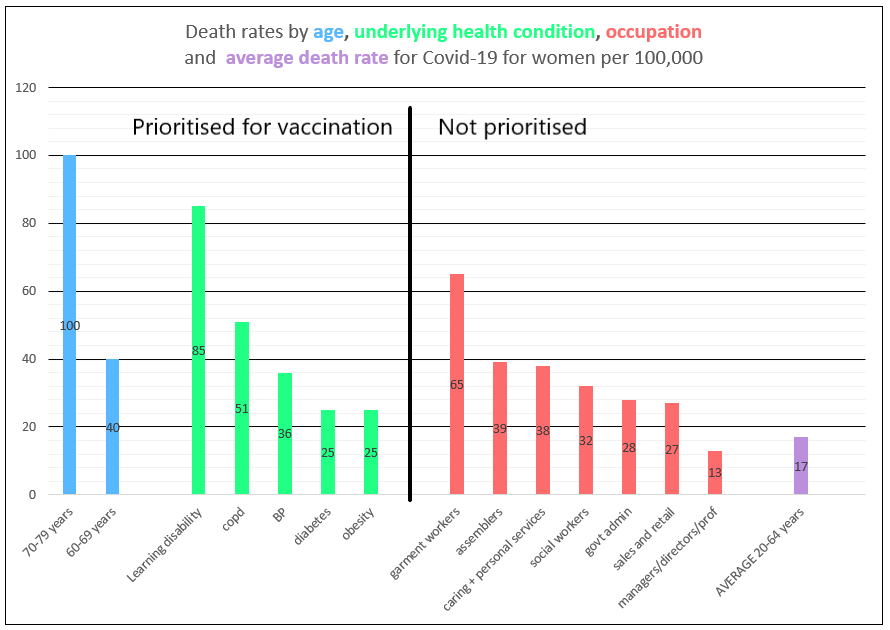
*ONS occupational categories are broad, for a detailed breakdown see here
JVCI has the following to say about occupational vaccination:
The committee considered evidence on the risk of exposure and risk of mortality by occupation. Under the priority groups advised below, those over 50 years of age, and all those 16 years of age and over in a risk group, would be eligible for vaccination within the first phase (i.e. all 9 priority groups) of the programme. This prioritisation captures almost all preventable deaths from COVID-19, including those associated with occupational exposure to infection. As such, JCVI does not advise further prioritisation by occupation during the first phase of the programme.
Occupational prioritisation could form part of a second phase of the programme, which would include healthy individuals from 16 years of age up to 50 years of age, subject to consideration of the latest data on vaccine safety and effectiveness.
This is moving the goalposts. JCVI cannot on the one hand argue that absolute risk of dying should determine priority when this is due to age and underlying medical condition, and then on the other hand say that risk of dying does not apply when it is due to occupational risk. The reasons behind the high death rates are surely irrelevant in terms of determining who gets priority for vaccination. If we are vaccinating people according to risk of dying, that is what we should be doing, across the board. The “first phase” referred to in the above quote, includes all 9 priority groups, and yes it will ultimately cover almost all preventable deaths (because it covers the great majority of the at-risk adult population i.e. over 38m people), but this will take many more weeks. One could apply the same logic to those with underlying medical conditions and advanced age, and say, “Don’t worry once we have vaccinated everyone over 50, you will also be covered, we don’t need to prioritise you”. That would clearly be nonsensical.
Many essential workers have death rates more than double those of people with underlying medical conditions and well in excess of people aged 65-69. It also cannot be right that a worker in a processing plant, and a senior manager or professional of the same age, have the same priority for vaccination, when the worker has over six times the risk of dying from Covid-19. Many essential workers are poor and many are black or Asian and it is striking that this double standard is being applied to them. One cannot imagine company directors and stockbrokers not getting vaccine priority if these death rates were reversed and they were the ones dying disproportionally from Covid-19.
The news that people with learning disabilities have now been prioritised for vaccination by the Joint Committee on Vaccination and Immunisation (JCVI) is to be warmly welcomed (Guardian 25 February 2021). The JCVI has done so “to ensure those most at risk of death or hospitalisation are prioritised” according to its statement, and a government source is quoted as saying “this is ultimately about who most likely to get seriously ill and die from this disease”. Why then have the JCVI and the government at the same time once again ruled out prioritising essential workers for vaccination, when their risk is also very high and certainly much higher than many people in groups 5 and 6 of the JCVI priority list who are now being vaccinated?
An equitable prioritisation programme of vaccinations demands essential workers should be immunised as the next priority group.
There are in addition several other important reasons for prioritising essential workers:
- While clear evidence of reduced transmission following vaccination is not yet available, early indications are that the vaccines do reduce transmission which is very much the hope of all of us, including the JCVI. If this does prove to be the case, immunising essential workers will have a greater impact on reducing transmission, because they are much more likely to live in overcrowded housing, and deprived communities where social distancing and other mitigation measures are more difficult. In addition, the more essential workers are protected the less transmission there will be in their workplaces which may be high risk, such as meat packing plants and garment factories.
- Although the great majority of deaths have been in people aged over 50, there have still been several hundred deaths of those under 50, and many thousands of Covid-19 infections in this age group, 5-10% of whom will have progressed to suffering debilitating Long Covid.
- There also appears to be a clear impression amongst front-line clinicians like Dr Helen Simpson that younger patients are getting sicker in the second wave, perhaps linked to the greater transmissibility and virulence of the new mutations. There is no data yet on this, but there have been a number of similar reports of patients in their 40s and 50s in intensive care recently.
- It will take many more weeks to vaccinate another 25m people, by which time many thousands of new infections will have occurred among essential workers because of their greater exposure, both to the public as part of their jobs, and/or to their fellow workers because of the nature of their work, and it must be said, poor compliance with health and safety requirements in the workplace by employers. Every week the PHE weekly surveillance report notes scores of outbreaks in the workplace; in the first week of February 2021 there were 112 workplace outbreaks reported to PHE.
- As noted above many essential workers are black or Asian and priority for vaccination would go a long way to protecting their families, especially those in overcrowded multi-generational households and the local community from the virus. This would be a very concrete way of addressing some of the large disparities in deaths suffered by black and Asian people, and send a clear signal that their lives matter to all of us.
- A nationally recognised campaign to immunise all essential workers would also make it plain to everyone, our collective appreciation of the role they have played throughout the pandemic on the front line, in ensuring that there is food, transport and essential services for all of us. Many essential workers are poorly paid and many are in precarious employment; offering them early protection against the virus would ensure they could continue working safely without putting the families and colleagues at work at risk.
- The recent report by the Joint Biosecurity Centre (JBC) states there is a “perfect storm” of factors, resulting in stubbornly high infection rates, which applies in deprived areas of the country: low wages, cramped multigenerational housing, failures in the test and trace service, lack of support for isolation, and public facing jobs. These factors are not going to be corrected any time soon, and vaccination would offer protection to these vulnerable workers and their communities.
- Without prioritisation, and a publicity campaign, many essential workers will end up not being vaccinated for all the usual reasons: poverty, reduced access to health care, language difficulties for many, etc. For once we could ensure that the “inverse care law” (those most in need get the least care) does not apply.
26 February 2021
References
Learning disability risk
Different figures have been published for death rates, but a government review of Covid-19 deaths of people with learning disabilities published in November 2020, stated an age and sex standardised death rate of 6.3 times the general population during the first wave of the pandemic. Black and Asian people with learning disabilities appear to have twice the death rate of white learning disabled people. The ONS recently reported the risk of death involving COVID-19 was 3.7 times greater for both men and women compared with people who did not have a learning disability, for the period January to November 2020. An average figure of five times the average risk has therefore been used for men and for women.
Risks for diabetes, COPD, hypertension and obesity have been calculated from the following sources and multiplying by average risk.
