
Feb 2021
CONTENTS
- Introduction
- Genetic “causes”
- Where does race and racism come from?
- Vitamin D deficiency
- Underlying medical conditions
- Unhealthy lifestyle
- Social class
- Structural or systemic racism
- Institutional racism
- Racism at the personal level
- “Weathering” – the effects of chronic stress from everyday racism
- Debunking the myths is important
- A note about the Sewell report
- References
1. Introduction
The death rate for black and Asian people in the UK from Covid-19 is three to four times higher than it is for white people. While many experts agree that exposure to the virus is important, others propose alternative explanations, such as genetic differences between races, lifestyle factors, and vitamin D deficiency.
In fact, the causes are very clear: as with almost all other diseases, poverty and racism determine who gets sick and dies most from Covid-19. The alternative explanations are simply distractions, do not stand up to scrutiny, and obstruct, confuse and delay efforts to address the underlying causes.
Lets look at these alternative explanations first.
2. Genetic “causes”
- There are about 25,000 genes in humans. Skin colour is determined by about 11 genes, [1] which are different and entirely separate from the over 1500 genes which determine immune function [2], and from the thousands of other genes which are responsible for the many physiological processes of the human body.
- There is no single gene or variant of any gene which is found in everyone of one “race” and not in people of another “race”.
- Genetic variation within races is greater than variation between races, so two people of different races may have more genes in common than two people of the same “race”.
- Medical research based on race has as much relevance or logic to it as research based on other physical characteristics like hair colour, height, or surnames beginning with the letter A for that matter.
- There are small genetic differences as a result of people’s geographic origin (like the sickle cell gene), or those which determine physical characteristics or cause genetic diseases like cystic fibrosis, but these are found in most populations to a greater or lesser degree. Race categorisation as the basis for biological research on the other hand, is “useless, pernicious nonsense”, to quote Mark Thomas, professor of evolutionary genetics at University College London.
- While race does not determine who we are genetically, it is very much a social reality, which affects income, housing, education, health, and many other aspects of how we live. Sociological research is therefore crucial to demonstrate the differences in outcomes in these areas for different racial groups, including the effects of racism in its various forms.
- More black people died in the UK in January 2021 (973 deaths) than in the Democratic Republic of Congo during the whole of the past year of the pandemic (712 deaths) with its population of 87 million people. The same is true of dozens of other African countries. Even allowing for substantial under-reporting, it is quite clear that death rates for Africans living in Africa are very much lower than those living in Europe and the US. “Something specific is happening to black people in US and UK”, as Dr Guddi Singh said on the recent BBC program “Why is Covid killing people of colour?”
- Some medical academics and official bodies in the UK lump together all Black and Asian people into “the BAME population”, and assign a “genetic cause” to their high rates of death from Covid-19. This is simply intellectual laziness and scientific illiteracy. What possible genetic defect could be common to billions of Africans and Asians across the world which miraculously only manifests in western countries where they are minority groups?
- People with learning disabilities have a death rate from Covid which is 4-6 times the average; these same academics would not dream of suggesting there is some genetic deficiency in their immune systems to account for this high mortality. The same is true of the 2.5 times higher death rate suffered by the most deprived 20% of population in the UK. They would not dare to suggest that poor people are genetically inferior and this is why they are dying at much higher rates. It is only society’s racialised thinking that makes them feel comfortable to speculate about genetic defects in Black and Asian people, a testament to the enduring nature of colonial attitudes, even among highly trained scientists.
3. Where does race, and racism, come from? *
- Race is not biological, it is a “social construct”, an invented, artificial system of categorising people and dividing us from one another based on skin colour.
- In 1758 a Swedish botanist Carl Linnaeus published a paper, categorising humans into four races: “red, white, yellow and black” corresponding to the Americas, Europe, Asia and Africa. The idea of different races was vigorously promoted by the colonial powers in the 18th and 19th centuries, who had of course already decided they were superior, and the red, yellow and black races were inferior. This was essential to justify the horrors of slavery, colonialism and exploitation. The real motives of economic greed and plunder, and political domination needed to be hidden, and white supremacy myths such as Rudyard Kipling’s “white man’s burden” of civilising the savages in the colonies, served this purpose well.
- European doctors, anthropologists and intellectuals gave crucial “scientific” justification to race theory, stating that those with darker skin colours were inferior, and this inferiority was inherent (what we call genetic today) and therefore unchangeable. Their “science” was often uncorroborated, pure racist prejudice, characterised by an absence of science, such as the collecting and measuring of skulls of colonised peoples to try and prove they had smaller brains.
- Some 35,000 men, women and children were brought to Europe and America from the colonies between 1800 and 1950, and then paraded before white Europeans and Americans in human zoos and circuses, and presented as “exotics, freaks and monsters and savages”. European scientists performed numerous studies on the people held in these zoos, publishing articles in scientific journals and laying the groundwork for race science and white superiority.
- Saartjie Baartman is perhaps the most famous of these victims, a young woman who was brought to Britain in 1810. Exhibited to demonstrate her large buttocks and labia for several years, the “Hottentot Venus” as she was called, made her owner a large amount of money before being sold to a French naturalist. After her death in 1815, her brain, skeleton and sexual organs were preserved and kept on display for another 160 years in the French Natural History Museum. Following a request by Nelson Mandela — and following fierce debate in the French National Assembly—her remains were returned and laid to rest in 2002 in her homeland in South Africa.
- This kind of dehumanisation, and its validation by race scientists, was, and is, needed to emotionally and intellectually anaesthetise white people to the dreadful things done to black people during empire and slavery, and to blame those who suffered most for their own misfortune.
- Race science reached its zenith in the Nazi policy of racial purity or eugenics, which resulted in the mass murder of millions of Jews, Gypsies and Slavs. We see the same demonising and dehumanising of immigrants who are seeking sanctuary in rich western countries today, and who are labelled by politicians and the tabloid press as criminals, terrorists and hordes bringing disease. This allows us to disregard their suffering, and their human rights, make living here as hostile and difficult as possible, lock them up indefinitely in detention centres and deport them back to countries they have fled from.
- Race based genetic research conducted today is simply the modern-day manifestation of scientific racism.
4. Vitamin D deficiency
- Vitamin D is involved to a small extent in immune function, and low levels of the vitamin are common in northern Europe, especially in the winter months when sunlight is limited. Whereas severe deficiency should be treated there is disagreement among experts about the importance of moderate deficiency of the vitamin Official advice in the UK is that the whole population should take daily supplements during winter, and people who have limited sun exposure (e.g. housebound people, those with dark skin or who habitually wear clothing leaving little of the skin uncovered), all through the year Supplementation is thought to offer increased protection against respiratory viruses in people with low Vitamin D levels.
- However there is no evidence that vitamin D deficiency causes worse outcomes in Covid-19 or that treatment with vitamin D is beneficial in the disease, whatever one’s skin colour. [4]
5. Underlying medical conditions
- The greatest risk factor for Covid-19 is age: there is a steep rise in mortality from seventy years of age. Those over 80 years of age have a 70 times higher risk of death of those under 40. Men have twice the mortality rate of women; the cause for this is not yet known; an interesting article on possible reasons for this can be found here.
- Many people have underlying medical conditions, which do confer additional risk in relation to Covid-19: for diabetes and obesity it is around a 50% increase, for cardiovascular disease the risk is doubled and for Chronic Obstructive Pulmonary Disease (COPD) it is around three times. Chronic kidney disease (CKD) is also a risk factor, people with very severe CKD have around 2.5 times the risk. [5]
- Black and Asian people in the UK do have higher rates of some of these chronic illnesses, but not to the extent that explains the additional risk of death. The ONS was quite clear on this in its October 2020 report: while underlying conditions do put people at additional risk, “ethnic differences in mortality involving COVID-19 …..cannot be explained by pre-existing health conditions…” [6]
6. Unhealthy lifestyle
- Obesity, smoking, activity/exercise levels, alcohol intake and unhealthy diet are clearly associated with poverty (particularly smoking and diet). There are variations in these individual factors but there is no evidence that overall they are significantly worse for black and Asian people.
- In addition, lifestyle factors themselves do not play a very significant role in Covid-19 mortality, apart from obesity (described above). Smoking carries a small additional risk; black and Asian people however smoke significantly less than the white majority in the UK.
Why are black and Asian people in the UK dying in such disproportionate numbers of Covid-19?
It is now clear that it is exposure to coronavirus that determines who gets infected. Exposure in turn is determined principally by the combination of social class and race.
7. Social class
People’s social class, i.e. their socio-economic circumstances, such as their occupation, housing conditions, educational level, income and resources, and access to health care and other services, has a major impact on their health and their life expectancy. Professor Michael Marmot has extensively documented this over the last 10 years; on average the most deprived, i.e. poorest 20% of people now live 8 years less than the richest 20%, and they also live with ill-health for 12 more years. In terms of Covid-19, as noted above people in the 20% most deprived areas have 2.5 times the death rate than those in the 20% least deprived areas, and at the peak of the 2nd wave in mid-January 2021 it was three times as high. [7].
8. Structural or systemic racism
In every area, socio-economic inequality and disadvantage are worse for black and Asian communities. This structural racism plays out in myriad ways. All ethnic minority groups are more likely to live in deprived neighbourhoods than white British people. [8] They are more likely to work in high-risk, often public facing jobs such as transport, health and social care and hospitality, and have zero hours, insecure jobs. They are more likely to live in overcrowded housing, to travel on public transport and to have fewer resources should they fall ill. Spread of infection within overcrowded households is much easier, including to vulnerable elderly relatives. Support for essential workers to self-isolate is inadequate, forcing people to choose between isolating or working and being able to feed their families and pay their bills.
This effect of this is seen in the ONS infection survey report in August 2020, which showed that on average all ethnic minority groups had over twice the infection rate of whites. [9] Being poor and black therefore carries a six times greater risk of infection with SARS-CoV-2 than being well-off and white.
Another ONS report published in October 2020 “Updating ethnic contrasts in deaths involving the coronavirus (COVID-19), England and Wales: deaths occurring 2 March to 28 July 2020” [10] is very helpful as it not only identifies those factors leading to higher death rates in ethnic minorities, but also calculates how much each factor contributes to the disproportionate death rates.
The ONS analysis adjusted the figures incrementally to reach the final figure for men and women in each ethnic group, according to “age, geography (local authority and population density), socio-economic factors (area deprivation, household composition, socio-economic position, highest qualification held, household tenure, multigenerational household flags) and occupation indicators (including keyworkers and exposure to others), and health (self-reported health and disability status in March 2011, and hospital-based comorbidities since April 2017).” The table below shows the results:
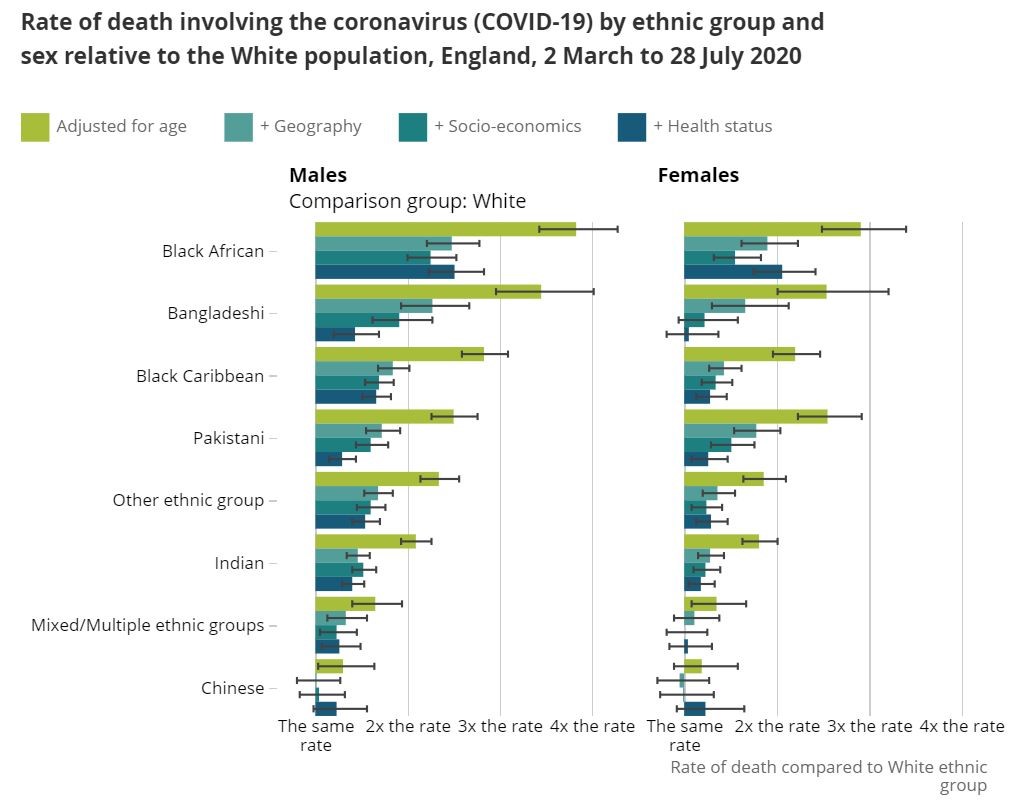
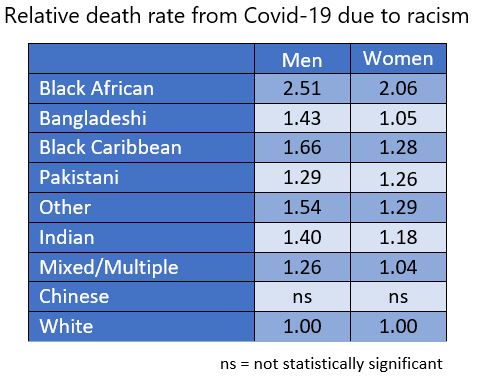
So, after adjusting for age, where people live, their socio-economic circumstances, their occupational exposure and their pre-existing health conditions, we see that every ethnic minority group still has a significantly higher death rate than white people, most marked for Black African men at 2.5 times the rate for White men, and 2.1 for women. While the ONS does not offer a reason for the enduring elevated death rates after correcting for the other known factors, thanks to its very detailed and meticulous work we are left only with the effects of racial discrimination. It is possible therefore to calculate “a racism death rate” for Covid-19 in the UK:
The ONS also found that “the relative differences between ethnic groups are larger for those younger than 70 years; the pattern is similar for males and females. This could be partly explained by the greater likelihood of the younger population being economically active and in employment.” The ONS also says that the results of its analysis in this report are in line with results from the Real-time Assessment of Community Transmission-2 (REACT-2) study, which indicate that different frequency of infection drive differences in mortality rates between ethnic groups.
The official SAGE committee, which gives scientific advice to the government on the Covid-19 pandemic, found that structural racism is central to the racial disparities in deaths from Covid-19. In a detailed report “Drivers of the higher COVID-19 incidence, morbidity and mortality among minority ethnic groups”, sent to the government on 24 September 2020, it stated, “All of these mechanisms (leading to racial disparities) arise from the wider social context that drive ethnic and other social inequalities, such as power relations and structural racism.” [11]
9. Institutional racism
The next layer of risk comes from things taking place within organisations and the workplace. This is the next level at which racism operates, i.e. day-to-day practices within the workplace, educational and other institutions and organisations, leading to greater exposure risk for black and Asian people.
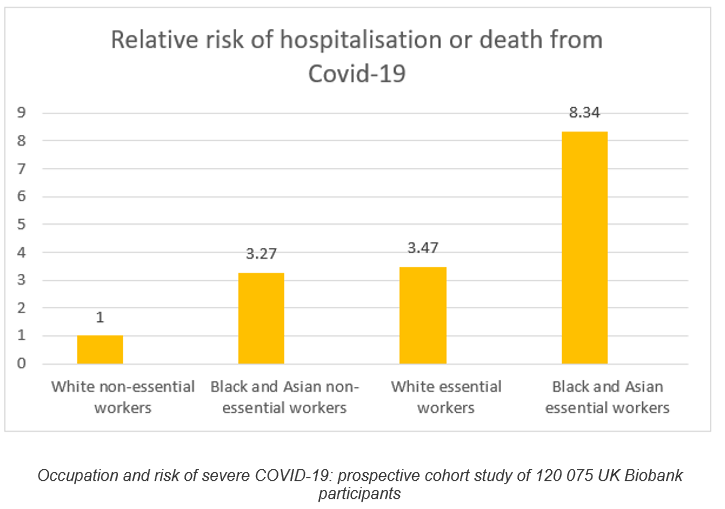
The effects of institutionalised racism on Covid-19 risk are clearly shown by the findings of the Biobank study [12] of 120,000 working age people, published in the BMJ in December 2020 – see table below. The study showed stark differences in risk of hospitalisation and death from Covid-19 between white and black workers and between essential and non-essential workers in the first wave of the pandemic. (Essential workers are health care workers, social care and educational workers, food, transport, police and protective services. Non-essential workers are all other categories of people in employment.) Once again we see the centrality of exposure in risk of Covid-19.
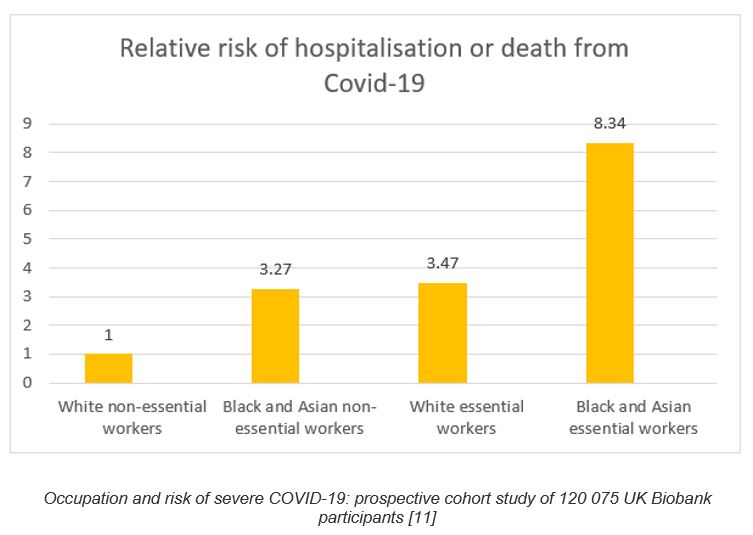
Adjusting for socio-economic factors, underlying health and lifestyle variables did not alter the risks. In other words we are talking about exposure to the coronavirus here. What is striking is not only the large difference made by occupation, but also how black workers have around 3 times the risk of white workers doing the same jobs. We also see how black or Asian workers who are not front-line, have the same risk as front-line white workers, and how black and Asian front-line workers have more than 8 times the risk of hospitalisation or death from Covid-19 than white non-essential workers. Race clearly adds a toxic additional layer of risk, by increasing exposure for black and Asian workers. How this happens is explored below.
Another study done in April 2020 at the University Hospital Birmingham [13] looked at SARS-CoV-2 seroprevalence (evidence of past infection) rates in different groups of health care workers (HCWs). It found hospital cleaners had the highest rate of infection (slightly higher than doctors and nurses on front-line Covid wards), and that for all grades of health care workers, black and Asian workers had nearly twice the infection rate of their white colleagues. The study also looked at socio-economic factors and found that although black and Asian HCWs did live in more deprived areas, this did not determine who got infected. The paper concluded: “the observed difference in seroprevalence rates…..is more likely due to occupational risk, rather than external factors.”
Disparities in death rates within the NHS among HCWs of different ethnicities are shocking. Black and Asian people make up 14% of the UK population, 21% of the NHS workforce but 63% of all deaths among NHS workers. Black and Asian doctors make up 44% of NHS doctors, yet they account for 95% of deaths of doctors from Covid-19. [14]
We see this same, disturbing fact over and over again: black and Asian people doing the same job as their white colleagues, but dying at 2-3 times the rate. This begs the question – what is going on in the workplace, and in our hospitals?
Testimony from nurses and doctors about the quality and availability of Personal Protective Equipment (PPE), as well as allocation of staff by management to frontline Covid wards, and workplace bullying, indicate a clear pattern of racism: a survey for Channel 4 News of black and Asian NHS staff found 61% felt they had unequal access to PPE, more than two-thirds (67%) reported feeling unsafe at work, and 50% said they did not feel able to speak up about safety in the workplace. “We are sandwiched between being bullied by raising concerns about lack of PPE and continued pressure to work at the frontline” said one respondent. [15] The BMA reported that almost double the proportion of BAME doctors (64 per cent) have felt pressured to work in settings with inadequate PPE. This compares with 33 per cent of doctors who identified as white. [16]
A TUC report into experiences of black and Asian workers’ experiences during the pandemic “Dying on the Job” [17] found that one in five BME workers said they received unfair treatment because of their ethnicity; around one in six BME workers felt they had been put more at risk of exposure to coronavirus because of their ethnic background. Many reported being forced to do frontline work that white colleagues had refused to do. Other respondents said they were denied access to proper PPE, refused risk assessments and were singled out to do high-risk work. The author of the report, Wilf Sullivan, the TUC Race Equality Officer, says, “This is not about black bodies, if white workers were exposed to the same extent as black workers it would have exactly the same effect”.
Just before the pandemic a separate ICM survey for the TUC of BME workers revealed that nearly half (45%) were given harder or less popular work tasks than their white colleagues. It also found racism was rife in the workplace: 31% of BME workers told the TUC that they had had been bullied or harassed at work; 32% had witnessed racist verbal or physical abuse in the workplace or at a work organised social event; 35% reported being unfairly turned down for a job; 24% had been singled out for redundancy and 15% of those that had been harassed said they left their job because of the racist treatment they received. Previous TUC analysis has found that BME people tend to be paid less than white workers with the same qualifications, and that they are more likely to work in low-paid, undervalued jobs on insecure contracts.
The position of migrants in high income countries demonstrates the way structural and institutional racism increase risk. Researchers at St George’s University found that, “In general, migrants have higher levels of many risk factors and vulnerabilities relevant to COVID-19, including increased exposure due to high-risk occupations and overcrowded accommodation, and barriers to health care including inadequate information, language barriers, and reduced entitlement to healthcare coverage related to their immigration status.” [18]
In a well referenced article in the Guardian on the occasion of the 72nd anniversary of the founding of NHS, Drs Bamrah and Chand document the many areas where racism operates within the organisation. They conclude: “So, the track record of the NHS on racism is poor. And although the NHS itself is not racist, its structural and institutional racism have blighted the lives of many BAME people….. It’s time to call time on racism in the NHS, and this would be its best birthday present.” [19]
NHS senior management are referred to as the “snowy white peaks” due to the overwhelming majority of senior management in the NHS being white. [20] The higher the pay band, the lower the proportion of BME nurses, midwives and health visitors. Across the 231 NHS trusts in England, in January 2019, only eight (3.5%) of chief nurses were of BME background while BME nurses comprise 20% of all nurses. The figures are a little better for doctors but not by much.
10. Racism at the personal level
Individual acts of racism in the workplace, in particular where there is an imbalance of power, may place black and Asian workers directly in harm’s way of Covid-19, as detailed in the TUC report. Tamira Harvey, daughter of Thomas Harvey, a Health Care Assistant who died of Covid-19 early on in the pandemic says he was failed in “multiple ways” in the BBC program. [14] She says he would complain of getting “flimsy PPE – a plastic apron and gloves” and he was ignored when he raised concerns at work about this because he was a black man. “Everyone has this idea in their head that the black man is strong and fearless and never gets ill; so I feel that played a part in him just being ignored and brushed to the side.”
11. Weathering: the effects of chronic stress from everyday racism
The internalised, physical and psychological stress of everyday racism also needs consideration in respect of the impact of Covid-19. It is well established that those that work or live in stressful environments, have a higher likelihood of many health problems, due to the chronic activation of the body’s stress response. [21] An ICM survey done for the Guardian in 2018 [22] of a representative sample of 3000 Britons, 1000 of whom were from ethnic minorities, laid bare the extent to which racism at a personal level is part of the daily lived experience of black and Asian people in the UK. It found that:
- 43% of those from a minority ethnic background felt they had been overlooked for a work promotion in a way that felt unfair in the last five years – more than twice the proportion of white people (18%) who reported the same experience
- ethnic minorities are three times as likely to have been thrown out of or denied entrance to a restaurant, bar or club in the last five years
- more than two-thirds of BME people believe Britain has a problem with racism
- 38% of people from ethnic minorities said they had been wrongly suspected of shoplifting in the last five years, compared with 14% of white people, with black people and women in particular more likely to be wrongly suspected
- minorities were more than twice as likely to have encountered abuse or rudeness from a stranger in the last week
- 53% of people from a minority background believed they had been treated differently because of their hair, clothes or appearance, compared with 29% of white people
- one in eight BME people had heard racist language directed at them in the month before they were surveyed, rising to 43% in the previous five years
- 57% of minorities said they felt they had to work harder to succeed in Britain because of their ethnicity, and 40% saying they earned less or had worse employment prospects for the same reason
- the poll persistently found evidence that the gap in negative experiences was not confined to the past, for example, one in seven people from ethnic minorities said they had been treated as a potential shoplifter in the last month, against one in 25 white people
- 41% of people said someone had assumed they were not British at some point in the last year because of their ethnicity
- people from minorities are twice as likely as white people to have been mistaken for staff in a restaurant, bar or shop; one in five said they had felt the need to alter their voice and appearance in the last year because of their ethnicity
Recalling being stopped and searched when he was 12, David Lammy MP said: “Stereotyping is not just something that happens, stereotyping is something that is felt, and it feels like sheer terror, confusion and shame.”
David Harewood, in the BBC program Why is Covid Killing People of Colour?, interviews Professor Arline Geronimus, who has long proposed the process of weathering. She says it’s not just that black people are more likely to get Covid-19, they are more likely to die of it at a younger age, and this is due to weathering, which in effect makes people biologically older than their chronological age. (This fits with the marked age difference in deaths and serious illness from Covid-19; black patients in ICUs are notably younger than white patients.)
Harewood describes how as a child “I would freeze, my whole body would tense and there would be a rush of adrenaline through my body” when racist abuse was shouted at him in the street on the way home from school. Harewood, who suffered a psychotic breakdown at the age of twenty-three, then speaks of the racism and discrimination black people have to face throughout their lives, and the cumulative effects of this. “It is exhausting, and wearying, it is literally weathering, eroding, the erosion of my sanity, it literally does just wear you out.”
Chronic stress is well known to have negative impacts on health, on a range of physical and mental disorders. “Stress induced immune dysregulation” can occur leading to impaired wound healing, cardiovascular disease and altered responses to infections and vaccinations. [23] The stress of dealing with everyday racism therefore may well also be contributing to increased Covid-19 deaths in black and Asian communities.
Racism is truly the other pandemic that black and Asian people are battling against in the UK, and like Covid-19, its impact is also devastating.
12. Debunking the myths is important
Clearly the causes of high death rates in black and Asian people in the UK are poverty and racism, which operate at different levels but are ever present, and together have been devastating for black and Asian communities
Other suggested causes, especially the suggested inherent defects in black and Asian people’s genes, their behaviour or their biology do not withstand scrutiny and are simply victim blaming. It is high time such preoccupations were abandoned by academics and government agencies and no longer attract research funding for investigation. Persisting with these “alternative explanations” or taking a “we do not know and we need more research” position are untenable stand points. Not only do they act to obscure the real causes of disparities in health but, intentionally or not, they also serve as a smokescreen that results in necessary remedial action being further postponed. After all, if the problem is in people’s genes, there is not much we can do about it.
There is another important reason. As Angela Saini says in her book “Superior: The Return of Race Science”, the acceptance of scientific racism has varied at different times with the prevailing political ideology. After the horror of WW2 and Nazi eugenics, these ideas became very unpopular, even taboo, but they were kept alive by a small group of academics, often funded by wealthy conservative institutions or think tanks. In the last few years, with the resurgence of right-wing populist politics in Europe and the US, the ideas of race science are once again entering main stream debate. And as in times of colonialism and slavery, race science serves to justify the actions of those in power and blame the weak, which we see in the harsh anti-immigrant policies of these governments, and the buttressing of white supremacy ideology.
The idle speculation of academics, that “there is likely to be a genetic cause”, is therefore not only unscientific, it is also deeply irresponsible. The scientific community should never forget the bloody history of race science, and it needs to stay true to the rigours of scientific enquiry and evidence-based findings. It needs to speak with one voice on this vital matter of our times. This will not only help educate the public about the real, social determinants of ill-health, it will also deprive white supremacy ideology of any scientific validation, and give policy makers and governments nowhere to hide when called upon to address these burning inequalities.
13. Postscript – a note about the Sewell report
This paper was completed just before the publication of a government commissioned report into “racial and ethnic disparities in the UK”, [24] by a panel chaired by Tony Sewell. Its findings are unsurprising given the well-known racism denialist views of Sewell and others on the panel, and is consistent with the government’s policy of denial and indifference to racism in the UK today, and as the historian David Olusoga says, the false choice it presents to the nation between addressing racial inequalities or class disadvatage.
The main contention of the report, that structural and institutional racism do not exist, is flatly contradicted by the SAGE report, as outlined above. (The SAGE report is not mentioned at all in the Sewell report, despite the fact that the committee has much greater expertise). The health section of the report has been roundly condemned by public health and primary care experts who state that it ignores decades of evidence of the causes of racial disparities in health. [25]
The Sewell report also suggests “genetic risk factors” as a cause of disparities in Covid deaths, which the SAGE report expressly also rejects, stating there is no evidence for such speculation. We have dealt comprehensively with this above. In the words of Lady Doreen Lawrence, mother of Stephen Lawrence who was murdered by white racists in 1993, the Sewell report “will give the green light to racists” in this country.
14. References
* With grateful thanks to Angela Saini, author of “Superior – the return of race science”. The section on the origins of race and racism draws heavily on her outstanding book.
[1] https://www.nature.com/articles/emm201228
[2] https://pubmed.ncbi.nlm.nih.gov/15780753/
[5] https://academic.oup.com/ndt/article/36/1/87/6041849
[9] quoted in SAGE report: Drivers of the higher COVID-19 incidence, morbidity and mortality among minority ethnic groups, page 5 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/925135/S0778_Drivers_of_the_higher_COVID-19_incidence__morbidity_and_mortality_among_minority_ethnic_groups.pdf
[12] https://oem.bmj.com/content/early/2020/12/01/oemed-2020-106731?utm_source=STAT#DC1
[13] https://thorax.bmj.com/content/75/12/1089
[14] https://www.bbc.co.uk/iplayer/episode/m000sv1d/why-is-covid-killing-people-of-colour
[16] https://www.bma.org.uk/news-and-opinion/bame-doctors-hit-worse-by-lack-of-ppe
[17] https://www.tuc.org.uk/research-analysis/reports/dying-job-racism-and-risk-work
[18] https://www.medrxiv.org/content/10.1101/2020.12.21.20248475v1
[19] https://www.theguardian.com/society/2020/jul/03/best-birthday-present-nhs-end-institutional-racism
[20] https://raceequalityfoundation.org.uk/wp-content/uploads/2018/02/Health-Briefing-39-_Final.pdf
[23] https://www.medicalnewstoday.com/articles/weathering-what-are-the-health-effects-of-stress-and-discrimination#Allostatic-load-much-higher-in-Black-adults and https://link.springer.com/chapter/10.1007/978-3-030-16996-1_6
